

Enamel regeneration gels are attracting a lot of attention because they promise something dentistry has never truly offered before: helping the tooth rebuild enamel-like mineral instead of only protecting what is left. If you have ever searched “dentist near me” because of sensitivity or white spots on your teeth, it is natural to ask: Is this real science, how far along is it, and when might it reach regular clinics?
In this guide, we look at what recent research actually shows, how these gels compare with fluoride, who might benefit most, and what realistic timelines and costs may look like. We also keep the focus practical: what you can do now to protect your enamel while labs test these new ideas. For a wider view of treatment options, you can explore the main dental services page or browse related articles on the Gold Coast Dental blog.
What Exactly Is Enamel Regeneration Gel?
Enamel regeneration gel is a protein-based or peptide-based dental gel designed to guide new hydroxyapatite crystal growth inside early enamel damage, creating an enamel-like layer on the tooth surface.
Unlike fluoride, which mainly hardens and protects the outer surface, these gels form a thin biomimetic matrix that behaves like the natural protein framework teeth used during development. The gel:
- Creates a scaffold on and inside early enamel lesions
- Pulls calcium and phosphate from saliva into that scaffold
- Encourages new mineral crystals to grow in the same direction as natural enamel rods
This approach sits under the umbrella of regenerative dentistry. You may see products described as “biomimetic enamel gel,” “protein-based enamel regrowth gel,” or “self-assembling peptide gel for enamel repair.” All share one aim: stabilizing early lesions and rebuilding a mineral layer that behaves more like real enamel.
How Much Can Tooth Enamel Really Regrow Today?
Your body does not naturally regrow fully lost enamel, but early enamel damage can now be remineralized and, in some cases, partially regenerated with targeted gels and fluoride-based care.
Current evidence supports three simple truths:
- Once enamel is completely worn through, the body does not replace it on its own.
- Early white-spot lesions and shallow demineralization can reharden with fluoride, nano-hydroxyapatite, casein-based creams, and self-assembling peptides.
- New enamel regeneration gels aim to build a more organized, enamel-like layer, but they are still in laboratory and early clinical stages.
That means most patients in the United States still rely on established tools:
- Fluoride toothpaste, rinses, and in-office varnish guided by professional recommendations
- Non-fluoride remineralizing agents such as nano-hydroxyapatite or CPP-ACP creams
- Conservative restorations when decay has gone beyond what remineralization can handle, such as tooth-colored fillings or crowns
If you want to see how enamel repair fits into overall treatment planning, you can review the full menu of care under cosmetic dentistry services or look at restorative topics in articles such as Dental Crowns: Types, Costs, and How Long They Last.
Lab Results: Before & After Enamel Growth 2026
Laboratory studies on extracted teeth show that protein-based gels can rebuild enamel-like layers within weeks, but these are controlled models, not everyday mouths.
Recent experiments on eroded human enamel samples found that a special elastin-like protein matrix could:
- Trigger ordered growth of apatite nanocrystals on damaged enamel surfaces
- Recreate micro-architecture similar to healthy enamel in different tooth regions
- Restore stiffness and hardness to levels close to intact enamel under simulated chewing
Clinical and in vitro work with self-assembling peptides has also shown that these gels can remineralize white-spot lesions more deeply than fluoride varnish alone and can help arrest early caries in permanent teeth. These “before and after” results explain the excitement around enamel regeneration.
At the same time, they should be read carefully. The fast changes often happen under controlled conditions on extracted teeth or in well-monitored clinical settings. Everyday life adds diet, saliva variation, plaque, and grinding, which may slow or limit how well these gels work. The fair summary is that lab studies suggest enamel-like repair can begin within weeks, but real-world timelines and success rates are still being mapped out.
How Do Biomimetic Gels Actually Regrow Enamel-Like Mineral?
Biomimetic enamel gels copy how natural proteins shape enamel during tooth development, then guide new mineral crystals to grow in the same direction.
The process usually follows four steps:
- Surface conditioning. A mild etch or conditioner opens tiny pores in the demineralized enamel so gel components can enter the lesion.
- Matrix application. The gel delivers short peptides or protein fragments that self-assemble into a nanofiber network, similar to the original protein scaffold in developing enamel.
- Mineral recruitment and growth. This network attracts calcium and phosphate from saliva and promotes new hydroxyapatite formation inside the lesion body.
- Hardening and integration. Over time, the new crystals align with existing enamel rods, increasing hardness and elasticity and creating a continuous, enamel-like surface.
For patients, the technical details boil down to a simple idea: instead of only sealing the surface, these gels try to rebuild from the inside out. Early caries, white-spot lesions, and shallow erosion are the best targets for this kind of treatment.
Enamel Regeneration vs Fluoride in 2026
Fluoride still has the strongest long-term clinical record, while enamel regeneration gels offer deeper repair for early lesions but remain newer and less tested.
Key differences include:
- Mechanism. Fluoride forms fluorapatite and slows mineral loss at the surface. Regeneration gels guide crystal growth inside the lesion and aim for more complete repair.
- Evidence for caries reduction. Community and school fluoride programs reduce decay in permanent teeth across populations, and fluoride toothpaste lowers risk when used daily. Recent reviews suggest that self-assembling peptide gels can outperform fluoride varnish alone for certain early lesions, especially white spots.
- Depth of effect. Fluoride works best on the surface and just below it. Peptide gels can reach deeper into early lesions, improving subsurface mineral density.
Most clinical guidance now views these approaches as complementary, not competing. An early lesion might be treated with a self-assembling peptide in the office and then maintained long term with fluoride toothpaste, periodic varnish, and regular dental checkups.
Can Enamel Regeneration Gels “Fix Teeth in 14 Days”?
Laboratory models on extracted teeth show enamel-like layers forming within one to two weeks, but there is not enough evidence to promise a “14-day fix” for everyday patients.
News stories often highlight the speed of enamel crystal growth in lab dishes. Those studies report that protein-based gels can create measurable mineral layers on eroded enamel samples within a matter of weeks and that these layers behave like natural enamel under mechanical testing.
In real mouths, the picture is more complex. Diet, saliva, oral hygiene, and tooth grinding affect how quickly lesions can stabilize and how much new mineral forms. Current clinical studies track early improvements over months, not days, and larger long-term studies are still underway.
A balanced message is that lab research suggests enamel-like repair can begin quickly under ideal conditions, but patients should not expect a guaranteed timeline or dramatic visual change in exactly 14 days.
Is Enamel Regeneration Gel Safe for Everyday Patients?
Early clinical data suggest a good safety profile for self-assembling peptide and protein-based gels, but long-term, high-frequency use in the general population is still being studied.
Trials on children and adults report good tolerance when these gels are applied to early enamel lesions under professional supervision. No serious adverse events have been linked to the peptide agents themselves in short- to medium-term follow-up.
Laboratory and ex vivo studies show that enamel surfaces treated with these biomimetic matrices remain stable under brushing and acid exposure. Some experimental systems also use keratin from hair or wool as a base for mineral coatings, which appears biocompatible in pilot work.
That said, regulators will still require longer follow-up on repeated courses of treatment, interactions with existing restorations and adhesives, and clear age guidelines. Until those questions are answered, many dental practices across the United States will reserve these gels for selected cases and will continue to rely on proven fluoride-based care for everyday prevention.
From Hair Protein to Tooth Coatings: The Keratin Story
A 2025 paper suggests that keratin from hair and wool can form an enamel-like mineral coating on teeth, opening a possible route to sustainable enamel repair products.
In that work, keratin was processed into a scaffold that binds calcium and phosphate and helps them crystallize into a closely packed mineral layer on demineralized enamel. The coating behaved like a protective shell in acid challenges and resisted wear under simulated brushing.
This strategy is interesting because keratin comes from biological “waste” materials, which may lower the environmental footprint of future enamel repair systems. However, keratin-based products are at a similar stage to other experimental gels: promising in the lab, still under evaluation for long-term performance and safety in real patients.
Clinical Evidence: What Do Human Trials Show?
Recent clinical trials and systematic reviews support self-assembling peptide gels as useful tools for early enamel lesions, but they do not replace fillings or crowns for deeper decay.
Clinical trials on noncavitated lesions show that self-assembling peptide gels can:
- Penetrate into early lesions and create measurable remineralization
- Reduce lesion depth and improve visual appearance under professional monitoring
- Perform better than fluoride varnish alone in certain white-spot and early occlusal lesions
Systematic reviews published in 2023–2025 conclude that these gels are promising noninvasive interventions for initial caries. They also stress that most studies have modest sample sizes and follow-up periods, so more data are needed before they become a primary treatment for all early lesions.
For patients, the takeaway is that enamel regeneration gels are already being studied in real people and can help the right kind of early lesion. They are not, however, magic erasers for every cavity in the mouth.
How Enamel Remineralization Works?
Early enamel weakening often begins with demineralization, a process caused by acids produced by oral bacteria after sugar consumption. These acids dissolve small amounts of minerals from the enamel surface.
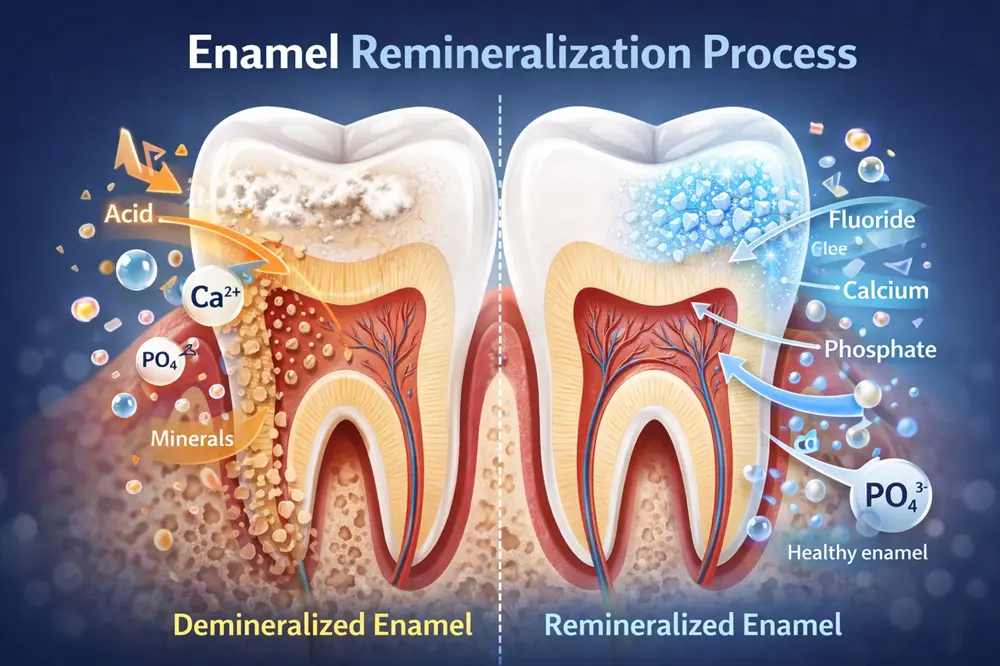
When saliva contains protective minerals such as fluoride, calcium, and phosphate, the tooth surface can absorb these minerals again through a natural repair process called remineralization. This process helps strengthen early weakened enamel and may slow or reverse very early stages of enamel damage before a cavity fully forms.
Can Enamel Regeneration Gels Eliminate Drilling?
They can reduce drilling for early lesions, but they will not remove the need for fillings, crowns, or root canals when damage is advanced.
Future noninvasive care may look like this:
- Early white spots and shallow lesions are treated with peptide or protein-based gels rather than immediate drilling.
- Dentists monitor the area at recall visits and only drill if the lesion keeps progressing.
- Fewer teeth need aggressive restorations over a lifetime because more problems are stopped early.
Once decay is deep, the tooth is cracked, or an old filling has failed, mechanical repair is still needed. That might mean a tooth-colored filling, an onlay, a full crown, or, in severe cases, a dental implant. You can read more about how these choices compare in articles such as Dental Implants vs Bridges: Benefits, Cost, Pros and Cons or learn about implant treatment options on the dental implants service page.
Projected Cost of Enamel Regeneration Treatment
Because these products are still emerging, cost estimates are based on today’s peptide treatments and early industry projections, not full fee surveys.
Many experts expect initial pricing in the range of USD $50–$150 per tooth or per localized treatment area, with variation based on:
- Whether the gel is applied in the office or as part of a supervised at-home kit
- How many teeth are treated at the same time
- What kind of imaging and follow-up appointments are needed
This places enamel regeneration gels between low-cost preventive options like fluoride varnish and higher-cost restorative or cosmetic treatments such as veneers or full crowns. As more data appear and codes are defined, insurers may start to cover part of the cost, especially when treatment prevents a more expensive restoration later.
When Might Enamel Regeneration Gels Reach Everyday Clinics?
Most observers expect limited use in specialized or early-adopter practices by the late 2020s, with broader access possible around 2027–2028 or later, depending on trials and regulators.
Several factors affect timing:
- Completion of multi-year clinical trials that track safety, durability, and patient outcomes
- Guidance from professional bodies and national dental organizations
- Reimbursement policies from insurers and public programs
Some products are already available in specific markets, but large numbers of general dentists will wait for clear guidelines on indications, age groups, and follow-up protocols. Until then, most practices will continue to focus on fluoride, sealants, and minimally invasive restorations as their main tools for caries control.
Who Is Most Likely to Benefit from Enamel Regrowth Technology?
Patients with early enamel damage and high sensitivity—not advanced cavities—are the main candidates for future enamel regeneration gels.
Groups that may benefit once these gels are widely available include:
- People with white-spot lesions after orthodontic treatment
- Patients with enamel erosion from acid reflux, frequent acidic drinks, or nighttime grinding
- Individuals with high caries risk but many lesions still in the noncavitated stage
- Adults who want to delay more invasive work by treating shallow enamel wear early
In contrast, people with deep cavities, large broken fillings, or teeth already weakened by repeated work will still need restorative care. Options such as crowns, veneers, and implant-supported restorations are described in more detail on the veneers service page and related cosmetic dentistry articles like Veneers: A Non-Invasive Solution for Stains, Chips, Cracks & Teeth Gaps.
Myths vs Facts About Enamel Regrowth
Myth: “Any toothpaste or gel that says ‘regrow enamel’ can rebuild fully lost tooth structure.”
Fact: Most over-the-counter products can reharden early enamel and reduce sensitivity, but they cannot replace large missing sections of tooth.
Myth: “Once these gels arrive, fillings and crowns will disappear.”
Fact: Enamel regeneration gels are designed for early lesions. Advanced decay and fractures still need mechanical repair with restorative materials.
Myth: “Natural home remedies alone can regrow enamel.”
Fact: Good diet and hygiene slow erosion and decay, but targeted agents such as fluoride, peptides, or other biomimetic materials are needed for meaningful remineralization and regeneration.
Scientific Comparison: Enamel Regeneration Gels vs Fluoride
Based on peer-reviewed studies up to late 2025; values reflect ranges from lab and clinical research, not guarantees for every patient.
| Aspect | Enamel Regeneration Gels (Biomimetic / Peptide-Based) | Traditional Fluoride (Varnish, Gel, Toothpaste) |
|---|---|---|
| Main action | Self-assembling matrix guides new hydroxyapatite crystal growth inside early lesions. | Strengthens outer enamel and slows mineral loss with fluorapatite formation. |
| Target lesions | Early noncavitated lesions, white-spot lesions, shallow erosion. | Broad use in both low- and high-risk patients for prevention. |
| Depth of effect | Reaches deeper into lesion body; can improve subsurface mineral density. | Strongest effect at and near the surface; limited subsurface regeneration. |
| Evidence (2023–2025) | Trials and reviews show improved remineralization versus fluoride varnish alone for selected early lesions. | Decades of data from community and home-use studies showing reduced caries rates. |
| Longevity (known) | Months to a few years in current data; long-term results still under study. | Safe repeated use across the lifespan when used as directed. |
| Safety profile | No major adverse events reported in early trials; long-term population data still building. | Well-supported safety record at recommended doses. |
| Typical setting | Dentist-applied or supervised use for selected early lesions. | Daily home use plus periodic professional application. |
| Key advantage | Potential to regenerate mineral inside early lesions and reduce drilling. | Low cost, strong evidence base, easy to integrate into daily routines. |
| Key limitation | Not yet widely available; evidence still maturing for everyday use. | Cannot repair deep structural damage or rebuild lost tooth structure. |
What You Can Do Now While You Wait for Future Enamel Gels
Even before enamel regeneration gels reach your local office, there is a lot you can do to protect the enamel you already have:
- Brush twice a day with fluoride toothpaste and clean between teeth daily.
- Limit acidic drinks such as sodas, energy drinks, and citrus juices, and avoid sipping them over long periods.
- Follow your dentist’s advice on fluoride varnish, sealants, and non-fluoride remineralizing agents if you are at higher risk.
- Ask whether early white-spot lesions or sensitivity areas might be candidates for future biomimetic treatments once they are widely approved.
If you are comparing options, you can read more about specific treatments in articles like The Best Ways to Prevent Teeth Stains and Enjoy a Whiter Smile or explore cosmetic options on the teeth whitening service page and the broader cosmetic dentistry section.
Closing & Call to Action
Enamel regeneration gels are moving from theory toward real-world care, but they are still in the early stages. The basics—good home hygiene, smart diet choices, fluoride, and regular checkups—remain the strongest tools for protecting your enamel right now.
Gold Coast Dental has over 19 locations across California and Texas, and our team follows evidence-based guidelines while tracking new developments in regenerative dentistry. If you are concerned about enamel wear, white spots, or tooth sensitivity, you can check our locations page to find your nearest Gold Coast Dental location, then call us now (562) 242-1411 .






